 Videos
Videos
 Quizzes
Quizzes
 Both
Both
Clinical case: Breast cancer development after prophylactic subcutaneous mastectomy
After reviewing this case you should be able to describe the following:
- What is meant by invasive ductal breast cancer.
- The relationship between BRCA genes and breast cancer.
- What is meant by accessory breast tissue, and how it relates to breast cancer.
This article is based on a case report published in the Journal "Case Reports in Surgery" in 2015, by Caroline C. Jadlowiec, Beata E. Lobel, Namita Akolkar, Michael D. Bourque, Thomas J. Devers, and David W. McFadden.
It has been modified and reviewed by Joel A. Vilensky PhD, Carlos A. Suárez-Quian PhD, Aykut Üren, MD.
Case description
History
The patient was a 46-year-old premenopausal woman who was concerned about a mass she felt in the left breast. Five years prior she had undergone bilateral prophylactic mastectomy because of a family history of breast cancer. The patient also had breast reconstruction via bilateral breast implants (Figure 2).
Physical examination
The patient, who had annual follow-up exams with ultrasound imaging, became aware of a mass in the lower quadrant of her left breast during the last month. The physical examination revealed a mass in the lower outer quadrant of her left breast near the edge of the implant in that breast.
Imaging
An ultrasound exam revealed an irregularly contoured solid lesion with dimensions of 1.3 x 1.5 cm. Follow-up MR imaging confirmed the presence of the lesion (Figure 3).
Histopathology and management
And, because the imaging was suggestive of a malignancy, a biopsy was ordered. The results of the excisional biopsy confirmed invasive ductal cancer. Based on this finding, an incision of 4 cm was made on the left lower quadrant, and the cancerous area was removed. Frozen section was performed during the surgery, and the surgical margins were found to be negative. An incision of about 5 cm long was also done in the axilla and the axillary lymph nodes were dissected and removed.
Evolution
The patient recovered well and was discharged and referred to the oncology department. The pathology report indicated invasive ductal carcinoma and reactive lymph nodes.
Surgical and anatomical considerations
Breast cancer risk and prophylaxis
In order to reduce their risk of developing breast cancer, prophylactic mastectomy is an option for high-risk women who have not yet been diagnosed with breast cancer. High risk factors for breast cancer include:
- a strong family history of breast and/or ovarian cancer
- a disease causing mutation in the BRCA1 gene or the BRCA2 gene
- a high-penetrance mutation in one of many other genes associated with the development of breast cancer.
Bilateral prophylactic mastectomy may include removal of both nipples (total mastectomy) or removal of breast tissue as far as possible while excluding the nipples (subcutaneous or nipple- sparing mastectomy). The latter procedure results in a more natural appearing breast than the total mastectomy procedure. However, total mastectomy is more preventive than the subcutaneous procedure because more breast tissue is removed. The patient in this case chose nipple and areola sparing mastectomy, which was one of the surgical options presented to her.
Prior to a prophylactic mastectomy a patient must be made aware of the associated possible risks inherent in this surgery:
- Bleeding or infection.
- Fluid accumulation under the scar.
- Delayed wound healing.
- Loss of breast sensitivity.
- Body image anxiety or depression.
Thus, even though the patient may avoid cancer, she still may suffer some debilitating consequences if she chooses prophylactic mastectomy.
Further, as shown by this case, mastectomy does not guarantee that breast cancer will never occur. Clearly, in this patient, the remaining breast tissue surrounding the implant became malignant. Even in total mastectomy, accessory breast tissue (e.g., in the axilla; see below) may develop cancer.
In this patient, the axillary lymph nodes were reactive, implying that the tumor was confined to the primary site and there was no metastasis to the lymph nodes.
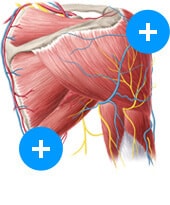
Prophylactic surgical procedure is typically the simple mastectomy, which removes only the primary breast tissue and leaves behind the axillary lymph nodes and anterior chest wall muscles. Therapeutic surgery for breast cancer is the radical mastectomy, which removes breast, related lymph nodes and pectoralis major and minor muscles (Figure 2). If the tumor does not involve the muscle layer, a modified radical mastectomy is performed, which removes only breast and related lymph nodes.
Sentinel node biopsy
Lymph from the breast drains to the axillary lymph nodes, draining first to the pectoral group, which is one of five axillary groups. Lymphatic system collects the lymph, which is derived from the interstitial fluid in all organs. Lymphatic capillaries are more permeable to large molecular weight proteins and large particles including bacteria and tumor cells compared to venous capillaries. This fluid eventually passes to lymph nodes for filtering. Lymph nodes thus are useful in determining whether cancer cells have metastases to other parts of the body.
In current breast cancer therapy a sentinel biopsy is done to determine if removal of the axillary nodes are necessary (Figure 5).
A sentinel lymph node is considered to be the first lymph node to which cancer cells would most likely to spread from a primary tumor. Sometimes, there can be multiple sentinel lymph nodes. A sentinel lymph node biopsy (SLNB) is a procedure in which the sentinel lymph node is identified, removed, and examined to determine whether cancer cells are present. A negative SLNB result suggests that cancer has not spread to nearby lymph nodes or other organs. A positive SLNB result suggests that cancer is present in the sentinel lymph node and may have metastasized to other nearby lymph nodes (called regional lymph nodes) and, possibly, other organs.
To determine the sentinel node the surgeon injects into the intercellular space near the tumor a radioactive substance or a blue dye, or both. This material flows to the sentinel lymph node. The surgeon then uses a device that detects radioactivity to find the sentinel node or searches for blue-stained lymph nodes that are stained. Once the sentinel lymph node is identified, a small incision (about 1 cm) is made in the overlying skin and the node is removed (Figure 5).
The sentinel node then undergoes a pathological examination. If cancer is found, the surgeon may remove additional lymph nodes, either during the same biopsy procedure or during a follow-up surgical procedure.
SLNB is usually done when the primary tumor is removed. However, the procedure can also be done prior to or after the excision of the tumor. SLNB may help some patients avoid more extensive lymph node surgery.
Objective explanations
Objectives
- What is meant by invasive ductal breast cancer.
- The relationship between BRCA genes and breast cancer.
- What is meant by accessory breast tissue why it is important relative to breast cancer.
Invasive ductal carcinoma
Invasive ductal carcinoma (invasive carcinoma) of no special type (NST) is the most common form of invasive breast cancer. It is a diagnosis of exclusion in that the cancer is not of a more spectacled type. The mammographic appearance of invasive ductal carcinoma is usually as a mass with fine spikes radiating from the edges (Figure 6). On breast examination, the lump of a malignant tumor typically feels much harder or firmer than benign breast lesions such as fibroadenoma. On pathological examination, the cancerous cells have invaded and replaced the surrounding normal tissues.
BRCA genes
BRCA1 and BRCA2 proteins are normally expressed from BRCA1 and BRCA2 genes (note that by convention the protein is printed in normal type whereas the gene is printed in italics) in many normal tissues of the body. However, inactivating mutations or loss of BRCA1 and BRCA2 result in higher risk of developing cancers in breast and ovary.
BRCA1&2 act to repair damaged DNA, or destroy cells if its DNA is beyond repair. If BRCA1 or BRCA2 are mutated, damaged DNA is allowed to replicate, and this is associated with an increased cancer risk. It is important to emphasize that BRCA1 and BRCA2 are normal; it is only when mutated there is an increased cancer risk. Women with an abnormal BRCA1 or BRCA2 have up to an 80% risk of developing breast cancer by age 90; they also have increased risk of developing ovarian cancer. Accordingly, women who have inherited mutated BRCA1 or BRCA2 may choose to have prophylactic mastectomies or may or undergo prophylactic chemotherapy.
The woman in this case had a family history of breast cancer and likely a defective gene. Unfortunately, her selection of a less than complete mastectomy allowed her remaining breast tissue to develop a malignancy.
Accessory breast tissue
Accessory breast tissue is a relatively common congenital condition in which breast tissue is found anywhere along the course of the embryologic mammary ridge (milk line; axilla to inguinal region; in humans, the ridge develops in the seventh week of gestation – this is prior to human sexual differentiation – thus, males as well as females have nipples).
Most women are unaware of their accessory breast tissue but the presence of this tissue may result in pain, milk secretion, thickening of the axillary skin and local skin irritation can occur (supernumerary nipples may also be present). Accessory breast tissue is sensitive to hormonal stimulation and thus may become more obvious during menarche, pregnancy, or lactation. And it is clinically significant that both benign and malignant diseases of breast tissue may develop in ectopic locations containing this accessory breast tissue. Furthermore, patients may develop cancer in this tissue even after total radical mastectomies.
Clinical case: Breast cancer development after prophylactic subcutaneous mastectomy: want to learn more about it?
Our engaging videos, interactive quizzes, in-depth articles and HD atlas are here to get you top results faster.
What do you prefer to learn with?
“I would honestly say that Kenhub cut my study time in half.”
–
Read more.
 Kim Bengochea, Regis University, Denver
Kim Bengochea, Regis University, Denver