 Videos
Videos
 Quizzes
Quizzes
 Both
Both
Femur
/images/vimeo_thumbnails/258827596/389fp8vOye1OLaezF09Wlw_overlay.jpg)
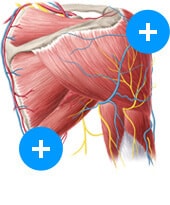
The femur bone is the strongest and longest bone in the body, occupying the space of the lower limb, between the hip and knee joints. Femur anatomy is so unique that it makes the bone suitable for supporting the numerous muscular and ligamentous attachments within this region, in addition to maximally extending the limb during ambulation. Proximally, the femur articulates with the pelvic bone. Distally, it interacts with the patella and the proximal aspect of the tibia.
The femur begins to develop between the 5th to 6th gestational week by way of endochondral ossification (where a bone is formed using a cartilage-based foundation). While several ossification centers (points of bone development) appear throughout intrauterine life, the bone continues to develop through childhood and early adolescence. Ossification of the femur is completed between the 14th and 18th years of life.
| Landmarks |
Proximal end - head, neck, greater trochanter, lesser trochanter, intertrochanteric crest Shaft - Borders: lateral and medial; Surfaces: anterior, medial, lateral; Ridges: lateral ridge (gluteal tuberosity), pectineal line, spiral line (these three lines converge and form the linea aspera) Distal end - lateral and medial condyles, intercondylar fossa, lateral and medial epicondyles |
| Joints |
Hip: femoral head with the acetabulum of the pelvis Knee: lateral and medial condyles of the femur with the tibial plateaus of the tibia (tibiofemoral joint); Patellar surface of the femur with the posterior surface of the patella (patellofemoral joint) |
| Blood supply | Trochanteric anastomosis, cruciate anastomosis |
| Disorders of the femur | Neck of femur fractures, slipped capital femoral epiphysis, femoroacetabular impingement |
This article will review the gross anatomy of the femur. It will also discuss the blood supply of the femur and summarize the points of muscular and ligamentous attachment. Additional discussion about clinical examination and disorders of the femur is also included.
Landmarks
Proximal end
The proximal end of the femur includes the:
- femoral head
- neck
- trochanters
- intertrochanteric crest
- intertrochanteric line
The head of femur is a roughly spherical structure that sits superomedially and projects anteriorly from the neck of the femur. The smooth convexity of the femoral head is disrupted on the posteroinferior surface by a depression known as the fovea for the ligament of the head (fovea capitis femoris).
Looking for a faster way to understand the anatomy of the femur? Our femur quizzes and diagram labeling activities are not only fast, but fun and effective, too!
This facilitates attachment of the ligament of the head of the femur (also called the ligamentum fovea or ligamentum teres). This ligament originates from the acetabular notch and accommodates the artery of the ligament of head of the femur. The femoral head forms the “ball” in the ball and socket joint of the hip. It is also located within the joint capsule and is covered by a synovial membrane.
The femoral neck is about 5 cm long and can be subdivided into three regions. The most lateral aspect (the part closest to the greater trochanter) is known as the base of the femoral neck or the basicervical portion of the neck is the widest part of the neck of the femur. The middle segment is also referred to as the midcervical part and is the narrowest part of the femoral neck. The most superomedial part is the subcapital portion; this is wider than the midcervical part but narrower than the basicervical segment. There are numerous foramina along the anterior and posterior surface of the neck of the femur to facilitate adequate blood supply.
The femoral head and shaft are situated at an angle of approximately 130 degrees. This neck-shaft angle (angle of inclination) is larger in infants and gradually decreases to the previously stated angle. It allows the limb to oscillate without colliding with the pelvis. Not only are there age-related differences in the angle of inclination, but there is also significant sexual dimorphism related to this anatomical feature as well. Genotypic females tend to have a wider angle of inclination than genotypic males do. This feature contributes to the difference in gait between the two sexes. The neck itself is anteverted (rotated laterally) at a variable angle between 10 – 15o (angle of torsion).
The superior margin of the femoral neck is nearly horizontal, with a concavity closest to the junction with the greater trochanter. The inferior margin is more oblique in orientation and projects posteroinferiorly and laterally toward the lesser trochanter. The posterior surface of the neck of the femur is directed posterosuperiorly. It is characterized by a longitudinal concavity and a transverse convexity, and the distal portion is located outside of the joint capsule. On the other hand, the anterior surface is flattened, located within the joint capsule, and meets the proximal end of the femoral shaft at the intertrochanteric line.
The femoral apophyses are prominent protrusions found on the proximal aspect of the femur. The lateral and larger of the two apophyses is the greater trochanter; its proximal edge is roughly a hand’s breadth inferior to the pubic tubercle on the pubis. The great trochanter is roughly quadrangular and extends from the superior aspect of the junction of the neck and shaft of the femur. It is associated with a crescent-shaped, rough, depression known as the trochanteric fossa, found on the medial surface of the apophysis. The lateral edge of the greater trochanter exists in continuity with the femoral shaft.
The medial apophysis is smaller, more conical, and extends in the posteromedial plane. It is called the lesser trochanter. While the apex and anterior aspect of the lesser trochanter are course to touch, the bony projection is smooth elsewhere. Unlike its larger counterpart, the lesser trochanter cannot be palpated.
There are two lines that connect the greater and lesser trochanters on the anterior and posterior aspect of the proximal femur. The intertrochanteric line is found anteriorly, while the intertrochanteric crest is found posteriorly. The intertrochanteric line starts anteriorly on a tubercle on the apex of the greater trochanter, near the intersection between the shaft and neck of the femur. It then travels inferomedially to a tubercle at the lower point of the lesser trochanter. The line then continues as the spiral line of the femur at the inferior aspect of the intertrochanteric line and continues into the medial lip of the linea aspera on the femoral shaft. It functions as the point of insertion for the superior and inferior bands of the iliofemoral ligament which is attached to the tubercle proximally and distally respectively.
On the other hand, the intertrochanteric crest is more pronounced than the intertrochanteric line. It is a pronounced ridge on the posterior surface of the femur, which begins at the intersection of the shaft and neck of the femur. It extends inferomedially from the greater trochanter to the lesser trochanter. Of note, the quadrate tubercle of the femur is also found along the intertrochanteric crest.
Shaft
The femoral shaft is a cylindrical structure with significant variability from one individual to another. The shaft is relatively wide at the proximal end but becomes progressively narrow toward the middle. It is bowed anteriorly, which contributes to the weight bearing capacity of the bone. The shaft then undergoes marked re-expansion towards the distal end. Anteriorly, the shaft is smooth and devoid of distinguishing features. However, the posterior surface is more rugged as it facilitates attachments of the large muscles of the thigh.
Although it is described as being a cylindrical structure, the shaft of the femur has several surfaces and borders that blend seamlessly. Toward the middle of the shaft, there are three surfaces and three borders. The convex anterior surface is bound by medial and lateral rounded borders. There is a posterolateral surface which is limited anteriorly by the lateral border and posteriorly by the linea aspera. There is also a posteromedial surface that is limited by the medial border anteriorly and by the linea aspera posteriorly.
There is a so-called third tuberosity in the form of the gluteal tuberosity. While it is not a true tuberosity, it may be large enough to be considered as such. It is rough and elongated along the long axis of the shaft; on the proximal posterior surface of the femur. The groove is continuous with the lateral lip of the linea aspera. On the medial, proximal, posterior part of the femur is another (smaller ridge) known as the pectineal line. It acts as the point of attachment for the pectineus muscle.
The most pronounced part of the posterior surface is the linea aspera. This is a raised longitudinal impression that runs along the long axis of the femur. It is made up of a medial and a lateral lip; the former originating near the lesser trochanter, and the latter arising from the greater trochanter. The medial and lateral lips unite along the middle third of the femoral shaft, traveling medial to the nutrient foramen.
The linea aspera then diverges toward the distal third of the femur where the medial and lateral lips become continuous with their respective ipsilateral supracondylar line (medial and lateral supracondylar lines). The medial supracondylar line continues to the adductor tubercle (on the medial condyle) and the lateral supracondylar line ends at the lateral condyle.
The popliteal surface of the femur is a triangular space found at the distal posterior surface of the femur. It is bordered medially and laterally by the corresponding supracondylar lines, and inferiorly by the superior border of the fibrous capsule of the knee. The caudal aspect of the surface forms part of the floor of the popliteal fossa.
Distal end
Not only is the distal femur the widest part of the bone, but it also interacts with both the proximal tibia and the patella. The distal end of the femur is made up of the medial and lateral condyles, the intercondylar fossa, and the patellar surface.
Complete your understanding of the interaction between the femur, tibia, and patella by learning more about the latter two bones using the following resources!
:format(jpeg)/images/study_unit/bones-knee-tibia-fibula/5LlbXZyjFaollWZ1YSUqA_Tibia_and_fibula.png)
Although the medial condyle is smaller than the lateral condyle, it is more readily palpable. It also accounts for the characteristic inward bulging at the knees. It is associated with a small conical protuberance known as the adductor tubercle, which provides a point of attachment for the large adductor magnus (powerful medial thigh muscle that moves the thigh medially). The medial epicondyle is situated below and anterior to the adductor tubercle. It also provides attachment for the tendon of adductor magnus muscle as well as the tibial collateral ligament (supporting structure connecting the tibia to the femur). The tendons of sartorius and gracilis muscles also pass over (but have no attachments) to the medial condyle of the femur.
Of the two condyles, the lateral condyle is larger and more prominent than the medial condyle. Like its counterpart, it is also associated with a lateral epicondyle, which functions as a point of attachment for the lateral collateral ligament. The lateral condyle also has a shallow groove below the lateral epicondyle through which the popliteal tendon travels. It is known as the groove for popliteus. There are three muscles that arise from the posterior aspect of the lateral femoral condyle. These are (from cranial to caudal) the plantaris muscle, the lateral head of gastrocnemius, and the popliteus muscle. The fibular collateral ligament (supporting structure that attaches the fibula to the femur) also has an insertion on the lateral condyle. It lies deep to the iliotibial tract (fibrous continuation of the tensor fasciae latae), which also inserts on the lateral femoral condyle.
While the medial and lateral femoral condyles are connected anteriorly, they are separated caudally by the intercondylar fossa. This groove is limited anteriorly by the patellar surface and posteriorly by the intercondylar line. It is a rough area with numerous vascular foramina to accommodate traversing vessels. While the fossa is located within the joint capsule, the majority of it sits outside of the synovial membrane. The medial wall of the fossa is formed by the lateral surface of the medial condyle, while the lateral wall is formed by the medial surface of the lateral condyle. Both walls bare indentations that accommodate the attachment of the cruciate ligament arising from the opposite side of the tibial plateau. In other words, the lateral surface of the medial condyle (the medial wall of the intercondylar fossa) serves as the point of attachment for the posterior cruciate ligament; while the medial surface of the lateral condyle (the lateral wall of the intercondylar fossa) bears an indentation for the anterior cruciate ligament. These smooth indentations are the only areas within the intercondylar fossa that are devoid of vascular foramina.
On the anterior surface of the distal femur, toward the anterior apex of the intercondylar fossa is an area known as the patellar surface or trochlear groove. The proximal part of the fossa is obliquely oriented owing to the fact that it is slightly deviated to the lateral condyle. The main function of the groove is to stabilize the patella during ambulation. As you can see, the femur can have a lot of anatomical landmarks.
If you want to learn them in an engaging way, take a look at our study unit:
:format(jpeg)/images/study_unit/anatomy-bones-femur/sOvBQnn2I4JxXiPw4ybYw_Femur_Thumbnail_06.png)
Mechanics
Humans are bipedal organisms–meaning that they are able to walk on two legs. The distribution of the weight of the organism is important in order to prevent trauma to supporting structures. The relationship of the femur with its proximal and distal articulations is rather unique. Firstly, the neck of the femur is angled superomedially in order to fit into the acetabulum. An ideal angle between the inferior margin of the femoral neck and the medial surface of the femoral shaft should be between 120 and 130 degrees. This angle of inclination ensures that the weight of the upper body passes along the mechanical axis of the femur. This axis can be identified by drawing a vertical line from the center of the femoral head to the center of a horizontal line across the tibial plateau (the center of the knee joint line). Please note that the mechanical axis of the femur differs from the anatomical axis of the femur (a line running from the center of the greater trochanter, along the femoral shaft, and ending at the center of the knee joint line).
The angle between the mechanical and anatomical axes of the femur is about 8 degrees. However, extreme variation of the angle of inclination could change this relationship and increase the amount of stress across the neck of the femur. The tibia also has a mechanical axis (the mechanical axis of the tibia) which runs from the knee joint line to the center of the ankle joint.
Both femurs naturally converge towards the knee. This degree of convergence is measured and recorded as the angle of convergence. Variation in the angle of convergence impacts the angle between the lateral aspects of the tibia and femur (the femoral-tibial angle, which is roughly 175 degrees). This measurement can be used as a surrogate for the gold standard for assessing the axial alignments, which is the hip-knee-ankle angle. Consequently, any extreme variation from this angle (such as those seen in varus and valgus deformities) will result in malalignment of the mechanical axes of the respective bones. Over time, the malalignment can result in the destruction of the joint surfaces and the progression of osteoarthritis.
Master the femur anatomy with our tailored quiz:
Joints
The femur has two important points of articulation that provide structural support for the body: the hip joint proximally; and the knee joint distally. Additionally, there are numerous supporting ligaments at both the proximal and distal articulations of the femur that provide added support to the joints. Please see the table below that summarizes the ligaments associated with each joint.
All three bones of the hip (ischium, ilium, and pubis) contribute to the formation of a relatively shallow concavity on the lateral aspect of the bone known as the acetabulum. The femoral head articulates with the hip via the acetabulum; giving rise to the hip joint (femoroacetabular joint). The ligament of the head of the femur is attached to the fovea (shallow depression on the superomedial part of the head of the femur) and to the center of the acetabulum. This joint is further reinforced by the pubofemoral and iliofemoral ligaments anteriorly, and the complex ischiofemoral ligament posteriorly.
The knee joint is a relatively unstable hinge joint formed by the interaction of three bones: femoral condyles articulate with the tibial plateau (tibiofemoral joint) and the patella (patellofemoral joint). This intricate combination of bones is further reinforced by numerous ligaments to enhance its stability.
The femoral condyles rest on very shallow, complementary depressions on the proximal tibial plateau known as facets. The depth of each facet is minimally enhanced by incomplete, cartilaginous rings known as menisci (singular, meniscus). The lateral meniscus is incomplete medially, while the medial meniscus is incomplete laterally. The free ends of each meniscus (the horns) are attached to the tibial plateau by ligaments. The tibial plateau also serves as the point of attachment for the anterior and posterior cruciate ligaments that insert on the contralateral wall of the intercondylar fossa.
Find out more about the anatomy of the hip and knee joints using the following study units:
:format(jpeg)/images/study_unit/anatomy-hip-joint/QIDFi4AcDDh5LRKoMon86Q_HipJoint_Thumbnail_05.png)
:format(jpeg)/images/study_unit/anatomy-knee-joint/6sTRcH8FR2KO3ouiyz298A_KneeJoint_Thumbnail_03.png)
The patella articulates with the patellar surface of the distal femur. This triangular bone is suspended within the tendon of the rectus femoris muscle from above, and the patellar tendon arising from below.
The interaction of these three bones requires numerous ligaments to prevent disarticulation (separation of the bones that interact at their joint). While the cruciate and meniscofemoral ligaments provide support within the synovial joint capsule, more robust ligaments are situated outside the capsule to keep the bones in line. The extracapsular ligaments supporting the knee are the two collateral ligaments (one on either side of the joint) and the patellar ligament (anteriorly). Posteriorly, the oblique popliteal ligament (which is a continuation of the tendon of the semimembranosus muscle) supports the joint capsule. The thigh muscles that cross the knee also provide additional support for the joint.
Consolidate your knowledge on the knee joint with the following quiz!
| Transverse acetabular ligament | Attached to the free edges of the acetabular labrum. |
| Ligament of head of femur | Attached to the fovea of the femoral head and the center of the acetabulum. |
| Pubofemoral ligament | Attached to the obturator crest and membrane, the iliopubic eminence, and the superior pubic ramus; blends with the iliofemoral ligament distally. |
| Iliofemoral ligament | Proximally inserted between the anterior superior iliac spine and the acetabular rim; distally attached at the intertrochanteric line. Also known as the Y ligament of Bigelow and the ligament of Bertin. |
| Ischiofemoral ligament | Arising from the greater trochanter to the ischium. Supports the joint posteriorly. Comprised of medial, lateral, and central bands. |
| Anterior cruciate ligament | Arising from the medial tibial eminence and inserting posteromedially on the medial wall of the lateral condyle. |
| Posterior cruciate ligament | Emerging from the posterior intercondylar area to insert on the lateral wall of the medial condyle. |
| Fibular (lateral) collateral ligament | Runs from the lateral femoral condyle to the head of the fibula. Blends with the tendon of biceps femoris but does not integrate with the joint capsule. |
| Tibial (medial) collateral ligament | Arises below the adductor tubercle of the medial femoral condyle to the medial epicondyle of the tibia. Integrates with the joint capsule. |
| Patellar ligament | Attached to the posterior surface and the apex of the patellar. Blends with the fibers of the tendon of rectus femoris anteriorly. Inserts on the tibial tuberosity. |
| Oblique popliteal ligament | Continuation of the tendon of the semimembranosus muscle. Supports the knee joint posteriorly. |
Blood supply
The blood supply of the proximal femur is of particular medical interest because of its susceptibility to damage. The so-called trochanteric anastomosis includes the medial and lateral circumflex femoral arteries (branches of the femoral artery) along with branches of the superior and inferior gluteal arteries. Branches arising from the deep femoral artery (also known as profunda femoris) also anastomose with both circumflex femoral arteries, as well as the inferior gluteal artery to form the cruciate anastomosis. They contribute to an anastomotic ring around the femoral neck.
Arising from the anastomotic ring are cervical arteries that pierce the joint capsule to become retinacular arteries. These retinacular arteries eventually form their own intracapsular anastomosis within the capsule. There is another – albeit minimal – blood supply arising from the obturator artery and traveling along the ligament of the head of the femur. The problem arises if there is damage to the neck of the femur; this could compromise the blood supply to the femoral head and lead to avascular necrosis.
The distal end of the femur has a rich blood supply arising from the popliteal vessels and the deep perforators. These vessels are not as vulnerable as those at the neck of the femur. Therefore the risk of avascular necrosis is negligible in this area. The femoral shaft receives its blood supply from nutrient arteries arising from the deep femoral artery.
All of the above arteries and branches can get extremely confusing, very fast! Especially with so many anastomoses taking place. Simplify your learning by taking a look at the following resources:
:format(jpeg)/images/study_unit/nerves-vessels-pelvis-thigh/bPpobjsf4ylP2RLelfbMw_Neurovasculature_of_the_hip_and_thigh.png)
:format(jpeg)/images/study_unit/the-femoral-artery-and-its-branches/oIbG70u70oXUUPLatpMIA_Femoral_artery_and_branches.png)
Muscle attachments
The femur is an integral component of ambulation. A lot of the large thigh muscles arise from and insert on the various parts of the femur. Muscles that originate from the pelvis and insert on the anterior or posterior surface of the femur to facilitate flexion and extension around the hips. Muscles which arise from the femur will cross the knee joint to insert on the proximal tibia promote flexion and extension around the knee. The tables below summarize the thigh muscles and their points of origin or insertion with respect to the femur.
| Iliacus and psoas major (iliopsoas) | Lesser trochanter |
| Pectineus | Pectineal line, linea aspera |
| Obturator externus | Trochanteric fossa of femur |
| Obturator internus | Medial surface of the greater trochanter |
| Superior and inferior gemelli | Medial surface of the greater trochanter (via tendon of obturator internus) |
| Piriformis | Apex of the greater trochanter (lateral and superior to the insertion of obturator internus) |
| Gluteus maximus | Iliotibial tract, gluteal tuberosity |
| Gluteus medius | Lateral aspect of the greater trochanter |
| Gluteus minimus | Anterior aspect of the greater trochanter |
| Quadratus femoris | Intertrochanteric crest |
| Adductor magnus |
Adductor part: Gluteal tuberosity, Linea aspera (medial lip), Medial supracondylar line Ischiocondylar part: Adductor tubercle |
| Adductor brevis | Linea aspera (medial lip) |
| Adductor longus | Linea aspera of the femur (medial lip) |
| Vastus lateralis | Linea aspera, greater trochanter |
| Vastus intermedius | Anterior surface of the femoral shaft |
| Vastus medialis | Intertrochanteric line |
| Articularis genu | Distal divergence of medial and lateral linea aspera |
| Biceps femoris brevis (short head) | Linea aspera (lateral lip), Lateral supracondylar line |
| Plantaris | Lateral supracondylar line of the femur, Oblique popliteal ligament of knee |
| Gastrocnemius |
Lateral head: Posterolateral surface of lateral femoral condyle Medial head: Medial femoral condyle, Popliteal surface of femoral shaft |
| Popliteus | Lateral femoral condyle, Posterior horn of lateral meniscus of knee joint |
Disorders of the femur
Trauma is the most common mechanism of injury for pathologies of the femur. However, there are other disorders that may arise from non-traumatic events (e.g. slipped capital femoral epiphysis or femoroacetabular impingement). Neoplastic disorders associated with the femur are excluded from this discussion.
Neck of femur fractures
The neck of the femur is the most vulnerable site for a fracture to occur. These fractures can be classified as intracapsular or extracapsular. The extracapsular fractures are also called basicervical fractures, while intracapsular fractures are transcervical and subcapital. The latter two carry the highest risk of resulting in avascular necrosis of the femoral head. The mechanism of injury is typically a high velocity from the distal end of the bone that is transmitted proximally. Alternatively, a fall from any height in an elderly patient may also result in a neck of femur fracture. A femoral neck fracture associated with low-velocity injuries often occurs on a background of osteopenia (decreased bone density); which may either be age or diet related.
Patients may provide a history of trauma and associated pain from the injury. There is often a history of difficulty in ambulation (which also exacerbates the pain) and an associated limb length discrepancy. The latter results from the fact that the affected limb may no longer be in the anatomical position as the injury may have caused rotational deformity or dislocation of the bone.
Slipped capital femoral epiphysis
On a histological level, the physis is an area of rapidly reproducing chondrocytes. The cartilaginous area is the point of growth for the expanding bone. However, in some individuals, the growth rate at the physis is too rapid and the interaction between the femoral head (proximal epiphysis) and the femoral neck is unstable. Therefore the head of the femur may ‘slip’ off of the supporting neck, thus the term slipped capital femoral epiphysis (or slipped upper femoral epiphysis) was coined. This disorder is more commonly encountered in pre-adolescent to adolescent males but can also be seen in females. While most cases only affect one side (the left more often than the right), it is not uncommon to see bilateral pathology. Other associated disorders such as obesity, endocrinopathies (like growth hormone abnormalities, hypothyroidism, and hypogonadism) have also been observed as predisposing factors to developing slipped capital femoral epiphysis. While these factors have been identified, a precise cause underlying these observations has not been found.
Patients may present with an acute onset of pain and inability to ambulate or chronic hip pain with pain being referred to the knees. In other cases, patients are known to have the disorder with an acute worsening of the slippage (acute on chronic). On examination, the affected limb is externally rotated when the hip is flexed and there may be limb length discrepancy. An anteroposterior plain radiograph of the pelvis will demonstrate loss of Shenton’s curve, Klein’s line, and obvious slippage of the capital epiphysis.
Clinicians may also want to entertain fractures of the neck of the femur or primary knee pathologies as possible differential diagnoses. Orthopedic surgeons opt to rectify this problem by pinning the capital epiphysis in place without reducing the displacement. The concern is that reducing the epiphysis to its original state may disrupt the delicate arterial anastomosis, leading to avascular necrosis of the femoral head.
Femoroacetabular impingement
Femoroacetabular impingement is a mechanical disorder characterized by hip pain with active and passive movements (particularly flexion and rotation) as a result of contact between the femoral head and the acetabulum. Over time, the recurrent wear and tear result in damage to the cartilaginous covering, leading to osteoarthritis. This disorder can be further classified based on the morphology of the bones involved. If the problem is due to an abnormal femoral head (aspherical head of the femur) then it is called a cam deformity. On the other hand, if there is an overgrowth of the acetabulum such that it hits the head of the femur during movement, then it is known as a pincer deformity. Of course, there are cases where both aspherical femoral heads coexist with overgrown acetabula. These situations are classified as mixed deformities.
Femur : want to learn more about it?
Our engaging videos, interactive quizzes, in-depth articles and HD atlas are here to get you top results faster.
What do you prefer to learn with?
“I would honestly say that Kenhub cut my study time in half.”
–
Read more.
 Kim Bengochea, Regis University, Denver
Kim Bengochea, Regis University, Denver