Overview of the heart valves and related structures.
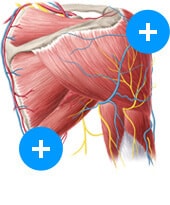
Heart in situ (anterior view)
Heart auscultation, and the lesser-practiced art of percussing the heart, are important aspects of a patient’s physical examination. Oftentimes, the vital signs of a patient, coupled with important details about blood pressure and heart sounds heard can be enough to lead to a diagnosis (after considering past medical history and other co-morbidities, of course).
Percussion of the heart involves tapping on the surface of the body in order to determine the underlying structure. More often, it is used as part of the clinical evaluation of the lungs and abdomen. However, percussion of the heart can be useful in estimating a patient’s heart size and/or pericardial effusion.
Auscultation is usually performed using a stethoscope, although louder heart murmurs and vascular abnormalities can sometimes be audible without the aid of a stethoscope. Auscultation of the heart can help gather an understanding of cardiac rate and rhythm, condition of the valves, as well as possible anatomical abnormalities, such as congenital defects or an underlying chronic condition.
The heart is enclosed in the chest cavity, within the rib cage, which allows for identifying the approximate location of the heart using the sternum and ribs as points of reference. Roughly 1 centimeter (cm) from the right sternal line, along the upper border of the 3rd right costal cartilage is the first point. Continuing to about 2.5 cm from the left lateral sternal line along the lower border of the 2nd left costal cartilage is the second point, which then forms the top boundary. The next point is found approximately 2 cm to the right of the sternum along the interspace between the 6th and 7th rib on the right, where the cartilage joins the sternum. The fourth and final point is found about 9 cm to the left of the midsternal line, and corresponds to the apex of the heart. Joining these points will form the other 3 borders of the heart.
The location where the 4 main heart valves can be heard is divided into the aortic area, pulmonic area, tricuspid area, and mitral area.
The aortic area is found in the 2nd intercostal space to the right of the sternum.
The pulmonic area is found in the 2nd intercostal space to the left of the sternum.
The tricuspid area is found in the 4th intercostal space to the left of the sternum, where other right heart sounds will also be heard.
Finally, the mitral area is found in the 5th intercostal space along the mid-clavicular line, where left heart sounds can also be heard.
These 4 areas can be remembered by the mnemonic “All Physicians Take Money” or “All Patients Take Meds”. Alternatively, some use the mnemonic Apartment M2245 (APT M2245), for the locations (2 right) aortic, (2 left) pulmonic, (4) tricuspid, and (5) mitral. Another important auscultation point is known as “Erb’s point” which is found at the 3rd left intercostal space, along the left sternal border, between the pulmonic and tricuspid areas.
For more details about the heart, take a look below:
Although palpation has largely replaced percussion in patient exams, it is nevertheless still useful. This is especially true when the point of maximal impulse (PMI), also known as the apical impulse, cannot be felt where the apex of the heart is located. The PMI will best be located with the patient in a supine position, near the 5th, or possibly 4th interspace along the mid-clavicular line. The PMI, if felt, will be accentuated in the left lateral decubitus position since this position displaces the apical impulse towards the left. Location, amplitude, and duration of the impulse should be noted at this point.
When the apical impulse cannot be palpated, percussion can be a useful option. Under these circumstances, cardiac dullness can occupy a large area, especially if there is a large pericardial effusion making the impulse undetectable. Cardiac percussion is performed starting at the very left of the chest, and percussing from resonance toward cardiac dullness in the 3rd, 4th, and 5th, and perhaps 6th interspaces, from the left axillary to the right axillary lines. Normal cardiac percussion should show dullness to percussion from the sternum to approximately 6 cm lateral to the left of the sternum.
Cardiac auscultation and auscultation points
A stethoscope is used for auscultation of the heart, and its head can involve one or two diaphragms that allow for low frequencies (the bell) or high frequencies (the diaphragm) to be heard. Some stethoscopes have a rotating head, where the bell is the smaller-sized end, and the diaphragm is the larger-sized end. For stethoscopes with diaphragms that allow dual-frequencies, the bell (low frequency) mode can be accessed by lightly resting the chest piece on the patient. When the diaphragm membrane is suspended, the membrane resonates the low-frequency sounds. To use the diaphragm (high frequency) mode, firm contact pressure is used to press the chest piece to the patient, such that movement of the diaphragm membrane is restricted. This way, the lower frequency sounds are blocked or attenuated, which allows for the higher frequency sounds to be heard.
Tricuspid valve (superior view)
To assess the heart sounds, we listen for rate, type, and rhythm of heart sound, as well as any sounds that are abnormal or additional, such as gallops, murmurs or clicks. Picking out heart sounds that deviate from the normal S1 and S2 sounds will take time. Heart sounds are most often described by the “lub-dub” sounds, which are the mitral and tricuspid valves closing (S1) during systole, followed by the closure of the aortic and pulmonary heart valves (S2) during diastole. S1 is best heard in the mitral area, and S2 is best heard at the left upper sternal border. Additional heart sounds are S3 and S4. S3 is heard in the early diastolic phase during rapid ventricular filling, which is associated with increased filling pressures (e.g., during heart failure or mitral regurgitation), or dilated ventricles. S4 is heard in late diastole, and is also known as the “atrial kick” due to high atrial pressure, where the left atrium must push against a stiff left ventricular wall. S4 is therefore associated with ventricular hypertrophy.
It is important to mention that there is normal splitting that occurs in regular heart sounds, which may be initially confusing. Normal splitting can be observed during inspiration, where breathing in causes a drop in intrathoracic pressure that leads to increased venous return. Increase venous return then results in increased RV filling, then leading to increased RV stroke volume, and finally increased RV ejection time, which ultimately leads to a delayed closure of the pulmonic valve. Therefore, S1 occurs first, followed by the A2, and P2 sounds.
Heart murmurs can be described by their duration, pitch, shape, and tonal quality, and can be accentuated by respiration and patient positions or bedside maneuvers.
The duration describes the portion of systole or diastole that the murmur occupies, and how long or short it lasts. A murmur that lasts throughout the entire duration of systole would be referred to as holosystolic or pansystolic.
The pitch of a murmur describes the frequency of the sound as high, medium, or low, where the diaphragm of the stethoscope is used for the medium and high pitched sounds, and the bell is used for the low pitched sounds.
A murmur can also be described by the sound’s shape, similar to the loudness and softness of notes in a piece of music. Common classifications include crescendo (increasing intensity), decrescendo (decreasing intensity), and crescendo-decrescendo (increasing then immediately decreasing intensity).
Finally, the murmur can be described by its tonal qualities, which includes the descriptions harsh, blowing, rumbling, clicking, sharp or dull. These tonal qualities oftentimes can offer a conjecture to the state of the valve. For example, a blowing sound is often heard during valvular regurgitation, when there is regurgitant backflow through a closed valve. A clicking sound is often heard when a valve is stiff and stenotic, where after blood has pushed against the affected valve with enough pressure, it will “snap” open with a “click” (or ejection sound) and the blood that rushes through then creates a “rumbling” sound due to the force of pressure it took to push open the stiff valve. “Dull” refers to a low frequency sound (such as a book dropping to the floor), while “sharp” refers to a high frequency sound (such as when a face is slapped). In general, a higher frequency sound will be heard through a smaller hole or gap.
Effects of respiration
It has already been mentioned that respiration can influence heart sound splitting. However, patient position can further intensify murmur sounds and allow for identification of which heart valve or area of the heart may be affect. Generally, murmurs sounds that increase with expiration originate from the left side of the heart (aortic or mitral valves), while murmurs increasing in intensity with inspiration originate from the right side of the heart (tricuspid or pulmonary valves).
To summarize this point again, inspiration increases right-sided heart sounds, and expiration increases left-sided heart sounds. A mnemonic for this is “RILE”: Right-sided – Inspiration, Left-sided – Expiration.
The mechanisms are as follows:
Right atrium (posterior view)During inspiration, there is a more negative intrathoracic pressure that pulls venous blood from the body into the heart. Similar the mechanism behind normal splitting, the increased venous return will result in increased RV filling. In addition, inspiration also reduces right atrial pressure. Simultaneously during inspiration, the lungs will be expanding, which causes the pulmonary blood volume to increase, therefore resulting in decreased blood flow away from the lungs into the left atrium. This means that right-sided heart sounds and murmurs will increase in intensity, whereas left-sided heart sounds and murmurs will decrease in intensity during inspiration.
Left atrium (posterior view)During expiration, the opposite happens where intrathoracic pressure will rise as the venous return decreases. Right atrial pressure will also increase during expiration. These processes result in decreased preload to the right side of the heart. With expiration, the lungs will be deflated, and more blood will flow from the lungs to the left atrium, which instead increases preload of the left side of the heart. Therefore, during expiration, left-sided heart sounds and murmurs will have greater intensity than right-sided ones.
Maneuvers
Bedside maneuvers can be used to accentuate heart sounds and murmurs for better identification and classification. These maneuvers can be grouped into 4 general groups based on physiological mechanisms. They are maneuvers that
increase preload
decrease preload
increase afterload
decrease afterload
Maneuvers that increase preload: squatting, passive leg raise, bringing the knee to the chest, or drugs that cause bradycardia or intravascular volume expansion (e.g., beta blockers)
Mechanism: Increased preload results in more blood available for the heart to pump through valves. With the increased venous return, there will be more blood flow on the right side of the heart. In general, the intensity of most murmurs will increase (e.g., mitral stenosis, aortic stenosis, mitral regurgitation, aortic regurgitation, ventricular septal defect), except for murmurs caused by mitral valve prolapse (MVP) and hypertrophic obstructive cardiomyopathy (HOCM). Any increase of blood inside the left ventricle will decrease MVP and HOCM murmurs due to the pathophysiology of these conditions.
Maneuvers that decrease preload: Valsalva (phase II) or standing up
Mechanism: Opposite of that explained for increased preload. The intensity of most murmurs will decrease, except for MVP and HOCM, which both increase in intensity.
Maneuvers that increase afterload: handgrip
Mechanism: Handgrip increases total peripheral resistance, similar to compression of the arteries of the arm, which will increase afterload. There is much less blood flow, such as in squatting, so there will be no increase in venous return. The increased afterload will make it harder for blood to flow forward from the left ventricle into the aorta, and therefore, there will be increased blood volume in the left ventricle. As a result, the decreased forward flow will mean there is a decrease in the intensity of forward flow murmurs (e.g., aortic stenosis), whereas, the intensity of regurgitant or backward flow murmurs will increase (e.g., mitral regurgitation, aortic regurgitation, ventricular septal defect).
Maneuvers that decrease afterload: amyl nitrate inhalation
Mechanism: Amyl nitrate has similar vasodilatory properties to nitroglycerin involving nitric oxide. However, whereas nitroglycerin is a potent venodilator, amyl nitrate acts as a potent dilator of arteries and arterioles. Therefore, the major effect of amyl nitrate is a decrease in afterload, which is dependent on arteries. Dilation of large arteries results in a decrease in total peripheral resistance that then decreases afterload and ultimately allows for increased forward flow of blood in the left side of the heart. It is worth mentioning that maneuvers affecting afterload does not affect ventricular filling during diastole.
In one last categorization:
Systolic heart sounds include aortic/pulmonic stenosis, mitral/tricuspid regurgitation, ventricular septal defect (VSD), and MVP.
Diastolic heart sounds include aortic/pulmonic regurgitation, and mitral/tricuspid stenosis.
Diagnostics and pathologies
Cardiac percussion
Cardiac percussion can be used in diagnosing several conditions:
Pericardial effusion can be identified by flat percussion over the lower half or two-thirds of the sternum in the absence of evidence for mitral stenosis.
Pulmonary hypertension, which is associated with dilation of the right ventricular outflow tract, is evidenced by marked dullness in the third left interspace.
Right atrial enlargement can be identified by marked dullness extending to the fifth intercostal space and sixth rib on the right of the sternum.
Right ventricular hypertrophy/dilation causes dullness over the sternum at the level of the fifth and sixth ribs, and extends to the left a few inches from the fourth intercostal space to the sixth.
Cardiac auscultation
Deviations from normal splitting can indicate possible pathophysiological states.
Wide splitting occurs in conditions that delay right ventricular emptying (e.g., pulmonic stenosis, right bundle branch blow), where delayed emptying causes a delayed pulmonic sound irregardless of breath.
Fixed splitting occurs in an atrial septal defect (ASD), where there is a left-to-right shunt of blood flow between the left and right atria that causes increased RA and RV volumes due to the higher left heart pressure gradient. Increased RA and RV volumes causes increased flow through the pulmonic valve, such that irregardless of breath, pulmonic closure will be greatly delayed.
Paradoxical splitting is such named for the abnormal reversed order of valve closure, where S1 is followed by P2 then the delayed A2 sound (instead of S1, A2, then P2). Paradoxical splitting is heard in conditions that delay aortic valve closure (e.g., aortic stenosis, left bundle branch block), where on inspiration, P2 closes later and moves closer to A2, thereby “paradoxicaly” eliminating the split.
Sources
All content published on Kenhub is reviewed by medical and anatomy experts. The information we provide is grounded on academic literature and peer-reviewed research. Kenhub does not provide medical advice. You can learn more about our content creation and review standards by reading our content quality guidelines.
Susan Standring, Gray's Anatomy: The Anatomical Basis of Clinical Practice, 41st edition, Elsevier.
Kenneth Saladin, Anatomy & Physiology: The Unity of Forma and Function, 6th edition, McGraw-Hill Science/Engineering/Math.
Anne M Gilroy, Brian R MacPherson, Lawrence M Ross and Michael Schuenke, Atlas of Anatomy, 2nd edition, Thieme.
Lynn S Bickley, Peter G. Szilagyi, and Barbara Bates. Bates' guide to physical examination and history taking, 11th edition. Philadelphia: Lippincott Williams & Wilkins.
 Videos
Videos
 Quizzes
Quizzes
 Both
Both
/images/vimeo_thumbnails/258660972/5G9A85KvfOrwAizsLM8JrA_overlay.jpg)
:format(jpeg)/images/study_unit/heart-in-situ/it8GNoFRI4UkNeAP29uYOA_Heart_in_situ.png)
:format(jpeg)/images/study_unit/heart-valves/0g9m4KGslN9kch6ZVT8PQw_Heart_valves.png)
:background_color(FFFFFF):format(jpeg)/images/library/1984/Xdg17EBOKwo1oYmnd62IJg_Atrium_dextrum_02.png)
:background_color(FFFFFF):format(jpeg)/images/library/1985/CF5MfxRBRmEvAbjNMphLQ_Atrium_sinistrum_02.png)
 Kim Bengochea, Regis University, Denver
Kim Bengochea, Regis University, Denver